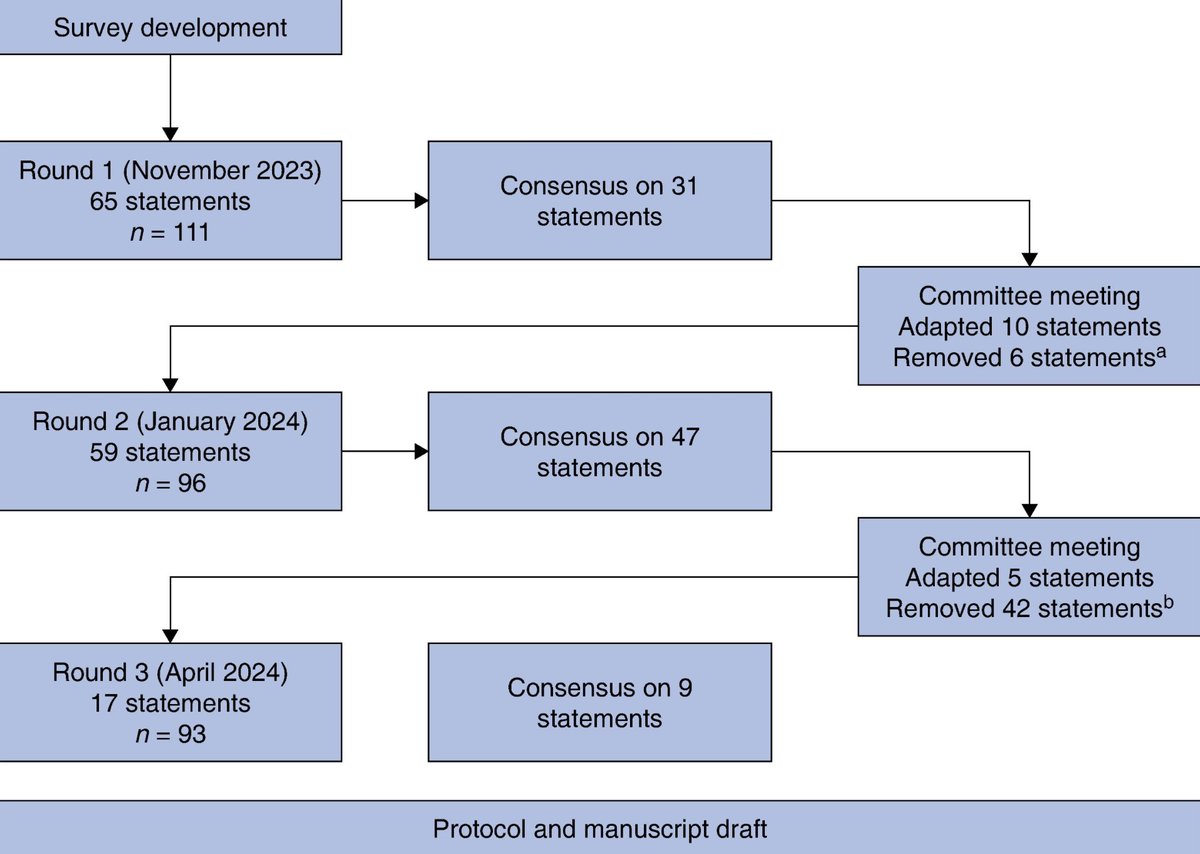
In late 2025, @MITFutureTech researchers conducted a #DelphiStudy to identify the most critical AI-related risks, vulnerable groups, and responsible parties. This year, they shared findings from the @MIT study that surveyed 272 global #AI experts to evaluate 24 AI risks, including likelihood, severity, vulnerability, responsibility, and overall concerns, over the next five years.
Among the top risks identified as a result of AI’s influence were market rivalry, weapons, cyberattacks, concentrated and consolidated AI control (economy, healthcare, civic engagement, etc.), the spread of false information, environmental harm, inequality, and unemployment.
The experts judged 18 of the 24 risks as having a probability of more than 10%, resulting in catastrophic outcomes (more than 1 million deaths and/or $100 billion in financial losses).
General public AI users were judged the most vulnerable to these risks, but experts assigned the highest responsibility for addressing them to general-purpose AI developers and governance professionals from both the public and private sectors.
Across most risks, experts identified information, finance, and national security as the most vulnerable sectors, which guide AI risk prioritization and clarify who is accountable for mitigation measures.
The biggest threat, in my view, is that the risks are unprecedented and involve too many unknowns to prepare for. As AI systems increasingly influence decisions in healthcare, employment, education, public safety, and democratic processes, it is crucial for citizens to support and actively promote strong human oversight and governance to ensure these systems benefit the public rather than control it.
We have a vital role to play in our part of the timeline by building a responsible AI framework, because future generations will only know and act based on what we leave them.
Follow #AINowSphere to access relevant #TechNews with clear insights related to AI, cybersecurity, and #EmergingTech topics.
cdn.prod.website-files.com/6…
#AIGovernance #Automation #EthicalAI #FutureOfWork #InfoSec #Innovation #MIT #MITFutureTech #NatSec #ResponsibleAI
32